
Written by: Matt Beucler, CEO, Plura AI
Key Takeaways for Healthcare Contact Center Leaders
- AI call centers for healthcare deliver ROI when organizations already handle at least 500 daily patient interactions across voice, SMS, RCS, and webchat.3
- Native HIPAA alignment, U.S. data residency, and FCC carrier ownership are baseline requirements for any platform that touches protected health information.1,2
- Stateful cross-channel memory keeps every patient journey connected so context follows the patient across calls, SMS, and webchat.
- Success depends on deep EHR integration via FHIR, clear human-escalation rules, and outcome metrics such as no-show reduction, not activity metrics alone.
- Ready to modernize patient communications? See how Plura’s HIPAA-aligned AI voice agents handle your specific patient interaction workflows in a live demonstration.
What Healthcare Organizations Prioritize in AI Call Centers
Operations and compliance leaders evaluating an AI call center for healthcare consistently focus on six criteria.
- Interaction volume threshold. AI agent platforms generate meaningful ROI at the 500-plus daily interaction level discussed earlier. Below that threshold, build cost and workflow design typically outweigh savings.
- EHR integration depth. Ninety-six percent of U.S. non-federal acute care hospitals use a certified EHR system, with Epic controlling more than half of acute-care multispecialty beds.4 Bidirectional integration via FHIR (Fast Healthcare Interoperability Resources) APIs is now the production standard. Agents that cannot read and write to the patient record create manual rework instead of saving time.
- HIPAA posture. The Health Insurance Portability and Accountability Act (HIPAA), codified at 45 CFR Parts 160, 162, and 164, covers the Privacy Rule, Security Rule, and Breach Notification Rule. Any vendor handling protected health information (PHI) should be prepared to sign a Business Associate Agreement (BAA) and demonstrate encryption, access controls, and audit logging. Customers remain responsible for their own HIPAA obligations and should consult qualified counsel for their specific situation.
- U.S. data residency. The FCC’s Notice of Proposed Rulemaking (NPRM, CG Docket No. 26-52) proposes capping offshore customer-service calls at 30% and limiting offshore handling of sensitive consumer data. Florida’s medical-information offshoring ban already restricts offshore handling of medical data at the state level.
- Human-escalation rules. AI agents need clear escalation paths. When a patient response falls outside the workflow’s scope, the agent should warm-transfer to a U.S. agent, flag the conversation in a unified inbox, or route to a designated escalation queue.
- Total cost of ownership. Traditional contact-center operations often run $4 million to $7 million annually. AI-driven platforms compress that range to roughly $300,000 to $700,000 on equivalent volume.3
How Healthcare Contact Centers Use AI Today
Healthcare call centers receive an average of 2,000 calls per day, and 60% of callers hang up if the phone is not answered within one minute. That pattern can represent up to $45,000 in lost revenue per day from a 7% abandonment rate.3 At the same time, physicians spend an estimated 4.5 hours per day on EHR documentation and related tasks, which reduces time available for direct patient care.
AI voice agents close this gap across five workflow categories.
- Appointment confirmations and scheduling. Automated outbound reminders and inbound booking flows reduce manual scheduling labor. Automated intake and documentation further reduce administrative hours.
- Patient intake and eligibility surveys. AI agents conduct structured intake interviews, including multi-question health-history surveys, and route only qualified patients to scheduling queues.
- Prescription reminders and medication adherence. Automated reminders from AI voice agents reduce missed appointments and support medication adherence programs.
- Revenue-cycle outreach. AI agents handle billing follow-up, eligibility verification, and claims-status updates at scale without adding headcount to the billing team.
- Post-care follow-up. Structured outreach after discharge captures patient status, flags deterioration signals for clinical review, and supports chronic care management.
The evaluation framework connects directly to these workflows. It tracks speed, such as sub-5-second first contact versus a 47-plus-hour industry standard, channel coverage across voice, SMS, RCS, and webchat, compliance posture across HIPAA, TCPA, and SOC 21,2, integration depth through EHR read and write via FHIR, and operational fit through escalation rules, human oversight, and audit logging.
Map these five workflow categories to your current patient interaction volume in a working session with Plura’s healthcare team.
AI Call Center Strategy for Healthcare Billing Teams
Healthcare billing teams have historically relied on two models. Onshore human agents carry full payroll, benefits, and turnover costs. Offshore BPO vendors reduce cost through wage arbitrage.
Both models now face regulatory and operational pressure. The FCC NPRM proposes limiting offshore handling of sensitive consumer data, including medical and financial information. The Keep Call Centers in America Act (S.2495) extends the federal regulatory perimeter. Florida’s medical-information offshoring ban and New York’s Call Center Jobs Act, with penalties up to $10,000 per day, already impose state-level restrictions.
AI voice and SMS tools appear to offer a third path. Many options fall short. Most are API resellers built on third-party CPaaS providers. These vendors do not own the carrier, cannot issue branded caller ID at the carrier level, cannot enforce real-time DNC scrubbing natively, and cannot hold conversation context across more than a single channel.
Plura AI operates differently. Plura owns its telecom infrastructure and holds an FCC carrier license, while competitors that depend on third-party CPaaS operate only as a software layer.4 Voice originates on Plura’s domestic infrastructure. The Stateful Conversation Database holds context across voice, SMS, RCS, and webchat, so a billing agent that sent an SMS about an outstanding balance at 9 a.m. can pick up a noon call already knowing what was discussed. All infrastructure is 100% U.S.-based by architecture, not by promise.
See how Plura’s pricing compares to your current billing team costs with side-by-side plan breakdowns.
Designing Healthcare Call Routing With AI
Healthcare call routing balances three tensions: automation versus human oversight, speed versus personalization, and channel mix versus auditability.
On automation versus oversight, Christopher Sharp, chief medical information officer at Stanford Health Care, notes that human review should remain central when using AI in EHRs.4 Humans review output and make final decisions. AI agents handle high-volume, low-clinical-risk flows. Human agents handle escalations, sensitive disclosures, and high-stakes clinical decisions.
On channel mix, shared conversation context across voice, SMS, RCS, and webchat now defines production-grade platforms. Platforms built on unified voice, messaging, and video infrastructure maintain shared context across touchpoints. Patients can start on a call and continue via SMS or web without repeating information.
Best practices for healthcare call routing deployments form a layered operational framework. Each layer builds on the previous one.
- Consent management. TCPA (Telephone Consumer Protection Act, 47 U.S.C. § 227) describes rules for outbound automated calls and messages. Consent records should be timestamped, immutable, and audit-ready. Organizations should consult qualified counsel for specific consent requirements.
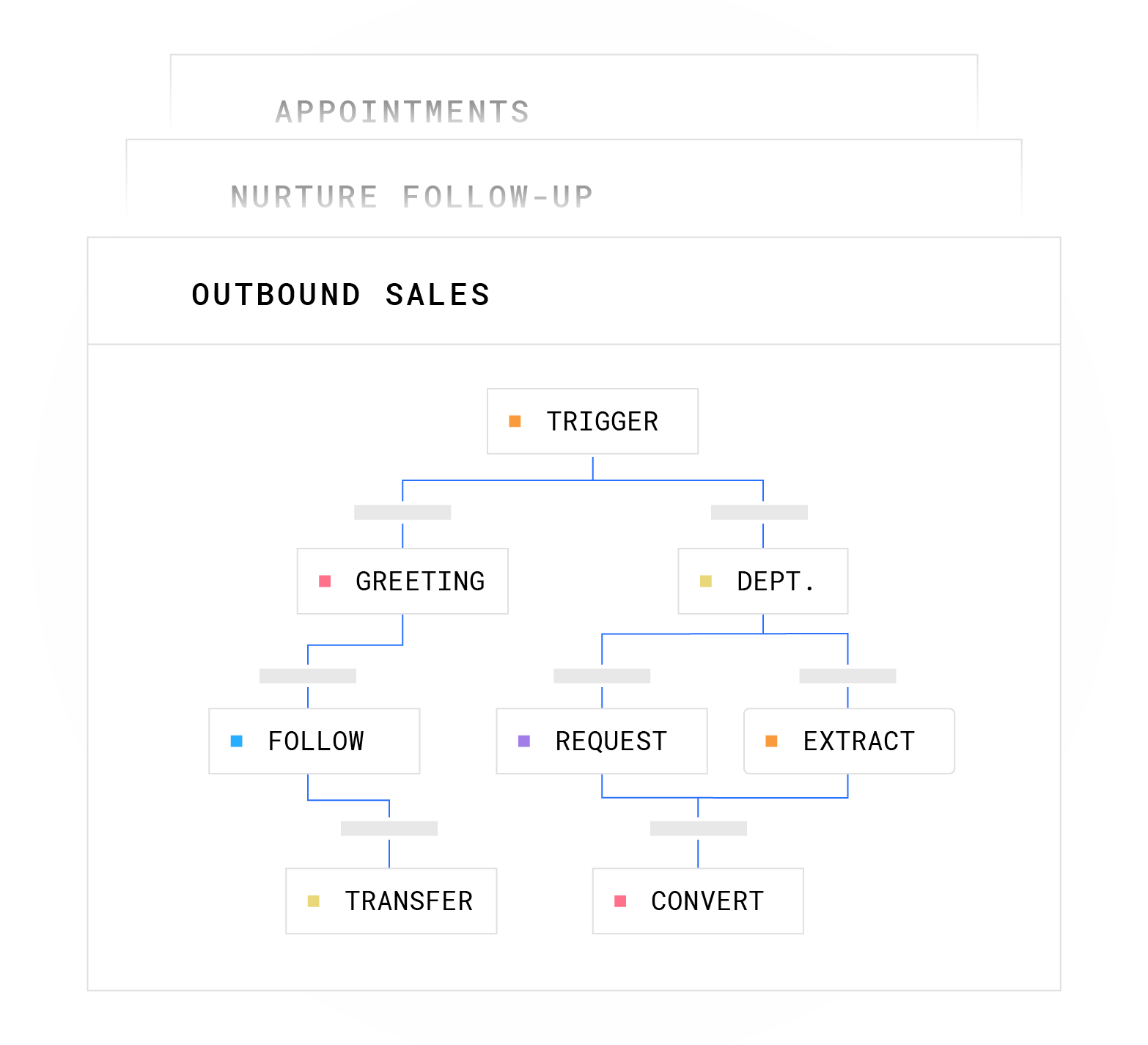
- Escalation paths. Every workflow node should carry a defined escalation trigger. Plura’s workflows include BATNA (best alternative to a negotiated agreement) guardrails that define the floor and ceiling within which an AI agent operates before routing to a human.
- Performance monitoring. Key metrics include average speed to answer, reduction in staff time on scheduling, error and rework rates in EHR documentation, and patient satisfaction scores. Reduced no-show rates and improved patient CSAT or NPS scores are recommended evaluation metrics for voice AI and EHR integration.
- SHAKEN/STIR authentication. SHAKEN/STIR (Secure Handling of Asserted information using toKENs / Secure Telephone Identity Revisited) caller ID verification runs on every outbound call. It confirms legitimate origination to the destination carrier and improves answer rates.
HIPAA-Aligned AI Call Center Readiness Checklist
Before deploying an AI call center for healthcare, operations and compliance leaders can review readiness across six dimensions.
- Minimum daily interaction volume. Organizations should meet the 500-plus interaction threshold referenced earlier to justify deployment investment.
- Process maturity. A disciplined rollout starts with baseline metrics such as hold times and abandonment rates and alignment across operations, IT, and physician leadership. Automating a broken workflow only produces a faster broken workflow.
- Data quality. AI agents read from and write to EHR systems via FHIR APIs. Incomplete or inconsistent patient records produce inaccurate agent responses. Seventy-one percent of U.S. hospitals used predictive AI integrated into their EHR systems in 2024. Satisfaction varies, which signals data-quality gaps that teams should address before AI agent deployment.
- Compliance requirements. Teams should confirm BAA readiness with the vendor, identify where PHI is processed, and verify that subprocessors for ASR, LLM, TTS, and telephony are covered by flow-down BAAs. HIPAA does not offer a certification program. Buyers instead select HIPAA-eligible vendors willing to sign a BAA and verify flow-down BAAs, data residency, and retention policies in writing. Customers remain responsible for their own HIPAA obligations.
- Internal ownership. AI deployments with engaged physician and nursing champions often achieve higher adoption than IT-only rollouts. Assign both a clinical owner and an operational owner before launch.
- Integration needs. Teams should map EHR touchpoints first. Define what the agent reads, what it writes, and which field mappings require clinical validation. Plura integrates with major EHR systems and supports more than 50 integrations across CRM, calendar, and data enrichment tools.
Healthcare organizations that complete this readiness checklist before deployment report meaningful operational outcomes. Plura’s healthcare deployments support up to 40% improvement in no-show rates through automated appointment confirmations and reminders.3
Quantify the ROI of meeting these six readiness criteria using your current interaction volume and staffing costs.
U.S.-Based AI Voice Agents in Healthcare: Common Pitfalls
Four deployment patterns consistently produce poor outcomes in healthcare AI voice agent rollouts.
- Automating broken workflows. AI agents execute workflows at scale. If the underlying scheduling logic, intake process, or billing follow-up sequence is broken, the AI executes the broken process faster and at higher volume. Teams should map and fix the workflow before automating it.
- Underestimating compliance complexity. Major U.S. hospital systems report spending $300,000 to $500,000 to vet and implement a single complex AI algorithm for healthcare use. Compliance operates as an ongoing discipline that touches HIPAA, TCPA, DNC, SOC 2, and many state rule sets. Plura supports customer compliance efforts through its built-in compliance engine. Customers remain responsible for their own regulatory obligations.
- Treating channels as separate systems. A patient who received an SMS about a billing balance and then calls the contact center should not need to re-explain the situation. Platforms that run voice and SMS as separate products with separate memories create friction at every handoff. Plura’s Stateful Conversation Database holds context across all four channels by default.
- Measuring only activity instead of outcomes. Call volume, handle time, and containment rate are activity metrics. The operational metrics that matter are no-show rate reduction, scheduling labor hours saved, claim denial rate, and patient satisfaction scores. Organizations often cite 24/7 availability as a key benefit of AI contact centers, and AI contact centers provide 24/7/365 availability that traditional offshore operations cannot match. Availability functions as an enabler, not an outcome, so teams should measure what that availability produces.
Frequently Asked Questions
How do AI communication systems differ from traditional contact-center tools?
Traditional contact-center tools route calls to human agents, log interactions in a CRM after the fact, and scale linearly with headcount. AI communication systems handle the conversation itself across voice, SMS, RCS, and webchat with shared memory across every channel. The key architectural difference is the Stateful Conversation Database. Every interaction is keyed to a patient token so the agent that sent an SMS at 9 a.m. can pick up the call at noon with full context. Traditional tools require the patient to repeat themselves at every handoff. Plura’s platform also runs on its own FCC-licensed carrier, which means branded caller ID, SHAKEN/STIR authentication, and real-time DNC scrubbing are enforced at the carrier level instead of bolted on through a third-party CPaaS.
What compliance considerations matter most for healthcare AI voice agents?
HIPAA’s three-rule framework, detailed earlier, governs any system that handles PHI. Vendors should be prepared to sign a BAA and demonstrate end-to-end encryption, role-based access controls, and tamper-proof audit logging. TCPA describes rules for outbound automated calls and messages, including consent documentation, opt-out mechanisms, and DNC list scrubbing. SOC 2 Type II reporting shows that a vendor’s security controls have operated effectively over a sustained period, not just at a point in time. U.S. data residency is increasingly material under the FCC NPRM and state-level laws in Florida, New York, New Jersey, Connecticut, and Missouri. Customers are responsible for their own compliance obligations and should consult qualified counsel for specific requirements.
How do omnichannel workflows function across voice, SMS, RCS, and webchat?
Omnichannel workflows in Plura operate through a single Stateful Conversation Database that all four channels read from and write to. When a patient receives an appointment reminder via SMS, confirms via webchat, and then calls with a billing question, the AI voice agent on that call already has the full interaction history. RCS enables branded, interactive messages with in-message documents and payments inside the message thread. Webchat reads the visitor’s page context in real time and tailors the conversation accordingly. The Unified Inbox gives human agents the same cross-channel view the AI uses, so escalations carry full context instead of starting from scratch.
What are typical implementation timelines for healthcare deployments?
Simple inbound qualification flows, such as appointment confirmations or prescription reminders, typically go live within days. Complex multi-step intake workflows, such as a 25-question health-history survey with conditional routing, often run closer to one to two months. The workflow logic requires design, clinical validation, and testing before production rollout. Plura’s onboarding sequence covers a discovery audit, intake of sample calls and existing scripts, an overnight build of a conversation mockup, a review and iteration session, engineering build of the production workflow, a pilot test on a subset of real calls, and full go-live. All annual contracts include a 90-day opt-out window.
How should organizations evaluate ROI of an AI call center for healthcare?
The ROI calculation starts with current contact-center cost, including headcount, hourly rate, taxes, benefits, commissions, and talk utilization. A 15-agent operation at $20 per hour with standard overhead and 40% talk utilization costs approximately $60,000 per month. Replacing that volume with Plura at $15 per hour, 100% talk utilization, and 6 AI agents doing the work of 15 humans drops the monthly cost to $14,400, a monthly saving of $45,600. Healthcare-specific ROI also includes no-show rate reduction, scheduling labor hours recovered, and claim denial rate improvement. Organizations can run their specific numbers using Plura’s calculator.
When is human handoff necessary in AI-driven patient interactions?
Human handoff becomes necessary when a patient response falls outside the workflow’s defined scope, when a sensitive clinical disclosure occurs, when a high-stakes objection or complaint requires judgment, or when the interaction involves a decision that carries clinical or legal risk. Plura’s workflows include explicit escalation triggers at every node. When a trigger fires, the AI warm-transfers the call to a U.S. agent with full conversation context, flags the interaction in the Unified Inbox, or routes to a designated escalation queue. The AI does not improvise on outcomes that matter. PHI and PII are redacted at the field level and routed through HIPAA-aligned channels throughout.
Conclusion: Turning Patient Conversations Into Measurable Outcomes
Healthcare organizations that handle at least 500 daily patient interactions have a clear path to deploying AI voice agents for scheduling, intake, triage, billing, and follow-up. The evaluation framework remains straightforward. Teams confirm interaction volume, EHR integration depth, HIPAA posture, U.S. data residency, escalation rules, and total cost of ownership before selecting a platform.
Architectural differentiators carry real weight in regulated healthcare environments. Carrier ownership, stateful cross-channel memory, and 100% U.S. infrastructure shape both risk and performance. Many AI voice tools on the market operate as API wrappers on third-party CPaaS providers. These tools do not own the carrier, cannot enforce compliance at origination, and cannot hold conversation context across channels. Plura AI owns its FCC-licensed carrier, runs all four channels on a single Stateful Conversation Database, and operates on 100% U.S. infrastructure by architecture. Plura supports customer compliance efforts across HIPAA, SOC 2, TCPA, DNC, and many state rule sets, while customers remain responsible for their own regulatory obligations.1,2
The common pitfalls are avoidable. Teams should avoid automating broken workflows, underestimating compliance complexity, treating channels as separate systems, and measuring activity instead of outcomes.
Run your numbers through Plura’s calculator to check your ROI in real time.
Compare plans and rates side by side.
Updated June 2026.
1 Plura AI maintains SOC 2, HIPAA, ISO, and GDPR posture as part of its platform infrastructure. References to compliance frameworks in this article describe Plura’s platform capabilities and do not constitute a guarantee that any customer using Plura will themselves be compliant with applicable laws or standards. Customers remain solely responsible for their own regulatory obligations, certifications, consent management, recordkeeping, and the claims they make to their own end users. Consult qualified legal counsel for guidance specific to your use case.
2 This article describes regulatory frameworks at a general level and does not constitute legal advice. Laws and regulations vary by jurisdiction, change over time, and apply differently depending on facts and circumstances. Readers should consult qualified legal counsel before making compliance decisions.
3 Performance figures, customer outcomes, and industry statistics referenced in this article are drawn from cited third-party sources or Plura customer case studies. Individual results vary based on implementation, use case, industry, audience, and execution. Past or aggregate performance is not a guarantee of future results.
4 References to third-party products, services, companies, or research are made for informational and comparative purposes only. Plura AI is not affiliated with, endorsed by, or sponsored by any third party named in this article unless explicitly stated. Trademarks and product names referenced remain the property of their respective owners.
This article is provided for informational purposes only and reflects Plura AI’s understanding at the time of publication. Product capabilities, integrations, and specifications are subject to change. For the most current information, visit plura.ai.
This article was produced with the assistance of AI tools and reviewed by Plura AI prior to publication.