
Written by: Matt Beucler, CEO, Plura AI
Key Takeaways
-
AI healthcare appointment scheduling automates booking, confirmation, and rescheduling across voice, SMS, RCS, and webchat while reducing no-shows by up to 40%.3
-
Two-way EHR integration via HL7 FHIR and multi-channel stateful memory keep patient context consistent across every touchpoint.
-
Platforms should support HIPAA, SOC 2, TCPA, and DNC compliance on 100% U.S. infrastructure to align with regulatory and data-residency expectations.1
-
Predictive no-show models and automated reminders improve attendance rates and free staff time for patient-facing work.
-
Teams can experience these capabilities firsthand by booking a live demo with Plura AI.
Five Capabilities Healthcare Leaders Expect From AI Scheduling
-
Automated booking, confirmation, and rescheduling across voice, SMS, RCS, and webchat
-
Predictive no-show identification and targeted outreach before the appointment window
-
Two-way EHR (Electronic Health Record) synchronization via HL7 FHIR (Fast Healthcare Interoperability Resources) APIs
-
Multi-channel stateful memory that carries patient context across every touchpoint
-
Infrastructure-level support for HIPAA, SOC 2, TCPA compliance, and DNC compliance on 100% U.S. infrastructure
Core Capabilities for Modern AI Scheduling
AI scheduling agents in 2026 operate as semiautonomous systems that handle the full appointment lifecycle.5 They manage initial booking, pre-visit confirmation, same-day reminders, and post-cancellation backfill.
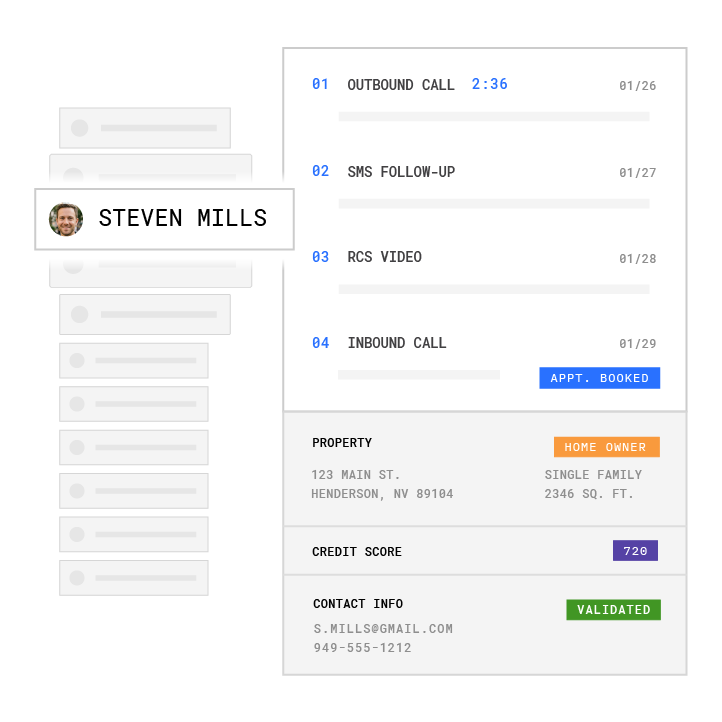
Plura AI agents run on four channels from a single platform: AI Voice, AI SMS, AI RCS, and AI Webchat.4 All four share a Stateful Conversation Database, so a patient who confirms via SMS at 9 a.m. does not re-explain themselves when the voice reminder arrives at noon. This cross-channel memory is possible because the platform runs on Plura’s own FCC-licensed audio bridging carrier rather than a third-party CPaaS (Communications Platform as a Service) like Twilio, which means branded caller ID is issued at the carrier level and SHAKEN/STIR caller ID verification authenticates every outbound call before it reaches the patient’s device.
Beyond simple appointment booking, some healthcare workflows require extensive patient qualification before scheduling can occur. Plura agents handle this complexity by conducting 25-question health-history surveys, redacting PHI (Protected Health Information) at the field level, and routing only qualified patients to scheduling queues. All of this happens within the same conversation thread that ultimately handles the booking.
Book a live demo with Plura to see the full scheduling workflow in action.
EHR Integration Realities for AI Scheduling
The multi-channel capabilities described above only deliver value when they connect cleanly to existing clinical systems. Two-way synchronization is the baseline requirement for any AI scheduling deployment. Bookings made by the AI must appear instantly in the EHR, and any staff changes to the schedule must be immediately visible to the AI to prevent double bookings and eliminate manual data entry between systems.
Data quality is the most common implementation risk. Incomplete, inconsistent, or legacy EHR data can reduce AI performance and reliability. Operations leaders should audit data completeness in patient records before go-live, not after. Workflow disruption during implementation is also documented. Staff resistance is a real barrier, and successful rollouts involve clinician input from the design phase.
Plura integrates with 50+ tools across CRM, calendar, and data enrichment categories. For scheduling specifically, the platform connects with Cal.com, Calendly, and Google Calendar, with EHR-specific integrations handled through the workflow layer and API connections documented in the integrations directory.
No-Show Reduction Tactics That Actually Work
No-show rates across U.S. healthcare settings remain significant. No-shows translate directly into unused capacity, higher per-visit costs, and lost downstream revenue.
Automated reminders via SMS and email reduce no-show rates by prompting patients to confirm in advance, and patients who complete that confirmation step are measurably less likely to miss their appointments.
These reminder-based interventions form the first line of defense against no-shows. Predictive models add a second layer by identifying which patients are most likely to miss appointments before the reminder window even opens.
Real-time schedule adaptation can also detect cancellations and automatically rebook slots by contacting waitlisted patients.

Plura delivers up to 40% improvement in no-shows by combining predictive modeling, multi-channel outreach, and automated backfill workflows.3
HIPAA and U.S. Infrastructure Considerations
Automation software that improves appointment scheduling or predicts no-shows qualifies as a healthcare operations activity under HIPAA and requires a Business Associate Agreement (BAA) when provided by a third-party vendor.
Core technical controls documented across the compliance literature include AES-256 encryption for data at rest, TLS for data in transit, role-based access control with MFA (Multi-Factor Authentication), immutable audit logs, minimum necessary data collection, and incident response procedures. Organizations should also map data flows for AI scheduling tools, including what PHI is ingested, where it is stored, who can access it, and how it leaves the system.
Multiple states impose requirements beyond the federal HIPAA floor.2 Several states require explicit consent before automated processing of sensitive data and prohibit sharing mental health, reproductive health, substance use, or genetic information with AI tools. Florida’s medical-information offshoring ban adds a specific restriction on offshore handling of patient data. Operations and compliance leaders should consult qualified counsel on state-specific obligations before deployment.
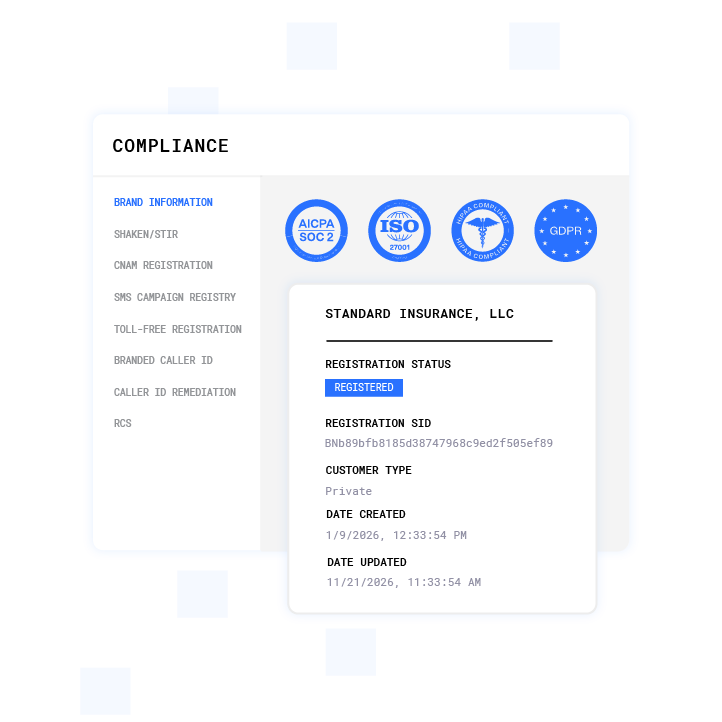
Plura’s infrastructure addresses the U.S. data residency dimension directly. Voice origination, model hosting, data storage, and call recording all run on 100% U.S. infrastructure, which reduces offshore exposure under the FCC NPRM (Notice of Proposed Rulemaking, CG Docket No. 26-52) and Florida’s medical-information offshoring statute. The platform supports compliance with HIPAA, SOC 2, ISO certification, GDPR (General Data Protection Regulation), SHAKEN/STIR caller ID verification, TCPA compliance, and DNC compliance.1 Plura provides the infrastructure, and downstream compliance obligations remain with the covered entity and its counsel.
Multi-Channel Stateful Memory in Practice
Most AI scheduling tools operate on a single channel with no memory of what happened on another. A patient who texted to confirm at 9 a.m. has to re-explain themselves when the voice call arrives at noon. That friction drives opt-outs and erodes the patient experience that scheduling automation should improve.
Plura’s Stateful Conversation Database addresses this at the architecture level. Every interaction across voice, SMS, RCS, and webchat is keyed to a patient token, typically a phone number or email, and persisted in one place. The AI reads and writes to that database on every conversation, referencing what was confirmed, what was declined, what is still open, and what sensitive data has been redacted. When a patient calls after receiving an SMS reminder, the voice agent already knows the appointment details, the patient’s confirmation status, and any prior objections raised in the text thread.
Value-based care models in 2026 incorporate omnichannel digital engagement tools and interoperability to create a unified patient experience across various digital platforms. Stateful cross-channel memory is the operational mechanism that makes that unified experience practical rather than aspirational.
RCS extends this further. Plura’s AI RCS channel delivers branded, interactive messages with rich media and in-message documents inside the patient’s native message thread, without redirecting to a web portal. Appointment confirmations, consent forms, and intake documents can be completed inside the conversation, with the response logged to the same stateful database the voice and SMS agents read from.
Vendor Evaluation Criteria for Healthcare AI Scheduling
Vendor evaluation for healthcare scheduling should focus on several non-negotiable items. These include BAA willingness and terms, SOC 2 Type II certification documentation, audit log retention and tamper-evidence capabilities, depth of two-way EHR synchronization, and whether the platform owns its carrier stack or rents from a third party. Vendors unwilling to sign a HIPAA-compliant BAA are described as unsuitable for PHI-touching workflows in the cited guidance, regardless of other capabilities.
Teams can compare plans and rates side by side on the pricing page.
Implementation Steps for AI Scheduling Rollouts
Once a platform meets the technical and compliance criteria, the next challenge is deployment. A structured deployment sequence reduces integration risk and compresses time to measurable outcomes. Plura’s onboarding sequence follows four phases:
-
Discovery (Week 1-2): Audit of existing scheduling workflows, call economics, EHR system, and sample call recordings. Identification of PHI data flows and integration points.
-
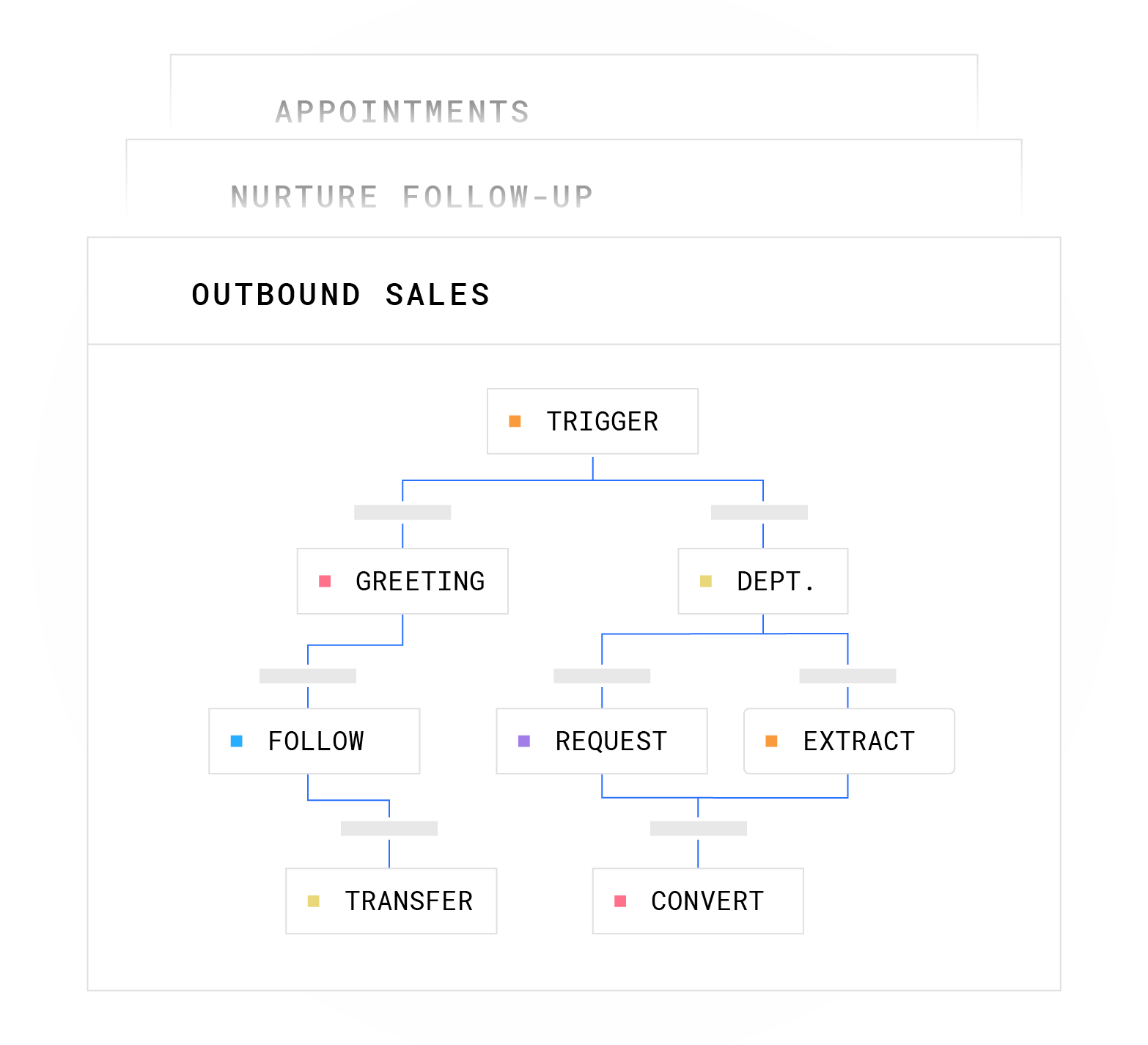
Build (Week 2-4): No-code workflow construction on Plura’s visual canvas. Conversation logic covers greeting, qualification, PHI redaction, confirmation, and escalation paths. BAA execution and compliance configuration occur in this phase.
-
Pilot (Week 4-6): Live deployment on a subset of appointment types or patient segments. Real-call monitoring against defined success metrics. Workflow iteration based on objection patterns and conversion gaps.
-
Go-Live (Week 6+): Full deployment across channels. Continuous conversation engineering with weekly tuning against outcome data. All annual contracts include a 90-day opt-out window if the deployment is not delivering.
Modern AI patient scheduling platforms with pre-built EHR integrations can be implemented and go live in a few weeks, though complex multi-step intake workflows run closer to one to two months because the conversation logic itself requires design and validation time.
Frequently Asked Questions
Which AI appointment scheduler fits healthcare needs in 2026?
The strongest platforms in 2026 combine multi-channel outreach across voice, SMS, RCS, and webchat with two-way EHR synchronization and stateful cross-channel memory.5 They also provide infrastructure-level support for HIPAA and TCPA compliance. Platforms that own their carrier stack rather than routing through a third-party CPaaS offer additional advantages such as branded caller ID, SHAKEN/STIR authentication at origination, and real-time DNC scrubbing enforced before each contact. Plura AI meets these criteria and runs on 100% U.S. infrastructure, which aligns with HIPAA data residency considerations and emerging state onshoring requirements. Evaluation should always include BAA execution, SOC 2 Type II documentation, and a pilot phase before full deployment.
Can AI handle appointment setting in a HIPAA-regulated environment?
AI appointment scheduling qualifies as a healthcare operations activity under HIPAA when the system handles PHI such as patient identifiers, visit reasons, and contact information. The key requirements include a signed Business Associate Agreement with the AI vendor, end-to-end encryption, role-based access controls, immutable audit logs, and minimum necessary data collection. Platforms that support these controls and provide SOC 2 Type II certification are appropriate for evaluation. Organizations remain responsible for their own HIPAA compliance obligations and should consult qualified counsel before deployment.
How much can AI reduce no-show rates in healthcare?
The evidence base shows meaningful reductions across multiple study designs. A 2025 JMIR Formative Research study at primary care centers found a reduction in no-shows after deploying an AI-driven scheduling and outreach system. As noted earlier, Plura’s platform achieves the 40% improvement benchmark through a combination of predictive modeling, automated reminders, and multi-channel outreach. Results vary by patient population, appointment type, and outreach cadence.
What does 100% U.S. infrastructure mean for healthcare AI scheduling?
100% U.S. infrastructure means voice origination, model hosting, data storage, and call recording all sit on domestic infrastructure with no offshore routing. This matters for two reasons in 2026. First, HIPAA data residency considerations and several state laws, including Florida’s medical-information offshoring ban, restrict offshore handling of patient data. Second, the FCC NPRM (CG Docket No. 26-52) proposes limiting offshore handling of sensitive consumer data, and the Keep Call Centers in America Act (S.2495) extends the federal regulatory perimeter. Platforms built on third-party CPaaS infrastructure cannot guarantee U.S.-only data routing because they do not control the underlying carrier. Plura owns its carrier stack, so U.S. infrastructure is an architectural fact, not a contractual promise.
How long does it take to implement AI healthcare appointment scheduling?
Simple inbound confirmation and reminder flows typically go live within a few weeks when the AI platform has pre-built EHR integrations. Complex workflows, such as 25-question health-history intakes with PHI redaction and multi-step qualification logic, run closer to one to two months because the conversation design and validation process takes time. The critical path items are BAA execution, EHR API access, data quality audit, and pilot testing on a representative appointment subset. Defining success metrics before launch, including no-show reduction targets, booking conversion rates, and after-hours capture rates, ensures the pilot phase produces actionable data rather than anecdotal feedback.
Conclusion
AI healthcare appointment scheduling in 2026 addresses a documented operational problem: no-show rates, administrative burden on front-desk staff, and patient communication that breaks down across disconnected channels. The platforms that solve this problem at scale combine multi-channel outreach, predictive no-show identification, two-way EHR synchronization, stateful cross-channel memory, and infrastructure-level support for HIPAA, TCPA compliance, DNC compliance, SOC 2, and SHAKEN/STIR caller ID verification on 100% U.S. infrastructure.
Plura AI delivers these capabilities from a single platform running on its own FCC-licensed carrier, with up to 40% improvement in no-shows and a 90-day opt-out window in every annual contract. The economics behind the deployment are transparent and the infrastructure is auditable.
Healthcare leaders can review detailed pricing and plan comparisons on the pricing page to find the right fit for their organization.
1 Plura AI maintains SOC 2, HIPAA, ISO, and GDPR posture as part of its platform infrastructure. References to compliance frameworks in this article describe Plura’s platform capabilities and do not constitute a guarantee that any customer using Plura will themselves be compliant with applicable laws or standards. Customers remain solely responsible for their own regulatory obligations, certifications, consent management, recordkeeping, and the claims they make to their own end users. Consult qualified legal counsel for guidance specific to your use case.
2 This article describes regulatory frameworks at a general level and does not constitute legal advice. Laws and regulations vary by jurisdiction, change over time, and apply differently depending on facts and circumstances. Readers should consult qualified legal counsel before making compliance decisions.
3 Performance figures, customer outcomes, and industry statistics referenced in this article are drawn from cited third-party sources or Plura customer case studies. Individual results vary based on implementation, use case, industry, audience, and execution. Past or aggregate performance is not a guarantee of future results.
4 References to third-party products, services, companies, or research are made for informational and comparative purposes only. Plura AI is not affiliated with, endorsed by, or sponsored by any third party named in this article unless explicitly stated. Trademarks and product names referenced remain the property of their respective owners.
5 This article contains forward-looking statements regarding industry trends, technology adoption, and future capabilities. These statements reflect current expectations and are subject to change. Plura AI undertakes no obligation to update forward-looking statements except as required.
This article is provided for informational purposes only and reflects Plura AI’s understanding at the time of publication. Product capabilities, integrations, and specifications are subject to change. For the most current information, visit plura.ai.
This article was produced with the assistance of AI tools and reviewed by Plura AI prior to publication.